
For years, orforglipron existed mostly as a promise, the GLP-1 drug you wouldn’t need a needle for. People talked about it the way they talk about a flight that keeps getting delayed. Then, on April 1, 2026, the FDA approved it under the brand name Foundayo, and the promise became a tablet you can pick up at a pharmacy [1]. The coverage practically wrote itself: no needle, no cold-chain ritual, just a pill.
That part of the story is true, and it matters. But spend enough time watching this drug class evolve, and a pattern starts to show itself. Every time a GLP-1 gets easier to take, somebody assumes it also got easier to manage. That has never actually been the case, and orforglipron is not about to be the exception. The format changed. The medicine underneath it, and the seriousness it demands, did not.
This piece follows that thread: how the supervision question got here, what it actually looks like in practice from the day you’re evaluated through the months it takes to see results, and, once you understand the standard, an honest look at who is actually meeting it. One fact worth carrying through all of it: orforglipron comes from a single manufacturer’s supply chain, Eli Lilly’s, so the supervised GLP-1 care most people can reach today runs through semaglutide and tirzepatide, with the same oversight standards expected to apply to orforglipron as telehealth access to it widens [1].
How the pill became the story, and why that’s the wrong story
It’s worth pausing on why the “just a pill” framing took hold so fast. Oral semaglutide, the prior attempt at a non-injectable GLP-1, came with real friction: an empty stomach, a small sip of plain water, a 30-minute wait before you could eat or drink anything else. Orforglipron doesn’t ask for any of that. Its approved label carries no food or water timing restrictions at all, it can be taken any time of day [1]. After years of that morning ritual being the price of an oral option, removing it is a genuine improvement, and it’s the kind of thing that keeps people on a daily medication for the long haul rather than letting it slip.
But convenience at the moment of swallowing a pill is a different question from what that pill does to your body over the following weeks, and that’s where the story gets more complicated than the headlines suggested. In the ACHIEVE-3 head-to-head trial, people actually discontinued orforglipron due to adverse events somewhat more often than they discontinued oral semaglutide, roughly 9 to 10% versus 5% [7]. Read that twice. The pill that’s easier to take produced more people quitting because of how it made them feel. The tablet solved a logistics problem. It did not solve the biology.
What good oversight actually looks like, from the first appointment onward
Before the first dose. Real supervision starts before anyone hands you a prescription. A licensed clinician has to actually look at your history, your current medications, your reasons for wanting the drug, and make a judgment call, not process an order the way a cashier rings up a purchase. That judgment matters more here than it would for an ordinary medication, because orforglipron’s label carries a boxed warning about thyroid C-cell tumors observed in rodents, and it’s contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 syndrome [1]. A clinician doing the job asks about exactly those things. If nobody asks, you haven’t been evaluated, you’ve been sold to, and that’s the clearest tell there is.
Honest providers also tell you what the pill isn’t. Tirzepatide, the strongest injectable in this class, has posted larger weight-loss numbers in its own pivotal trials, and a clinician worth paying will say so upfront, telling you when the shot might get you further than the tablet will, even if the tablet is more convenient day to day [3]. That’s not a conversation a good provider waits to be asked. They volunteer it.
The first weeks, where most of the damage is done or avoided. Nobody starts orforglipron at full strength. The dose climbs in steps over weeks, precisely because climbing too fast is how the class’s known side effects, mostly nausea, vomiting, and diarrhea, become severe enough that people stop taking the drug altogether [1][3]. Good supervision through this stretch means pacing the increase to how you’re actually tolerating it rather than a fixed calendar, being reachable when something feels off, and being able to tell you whether that feeling is the expected adjustment or a signal worth acting on. Given what ACHIEVE-3 showed about discontinuation rates, this is not a phase to go through with a stranger on the other end of a chat window [7].
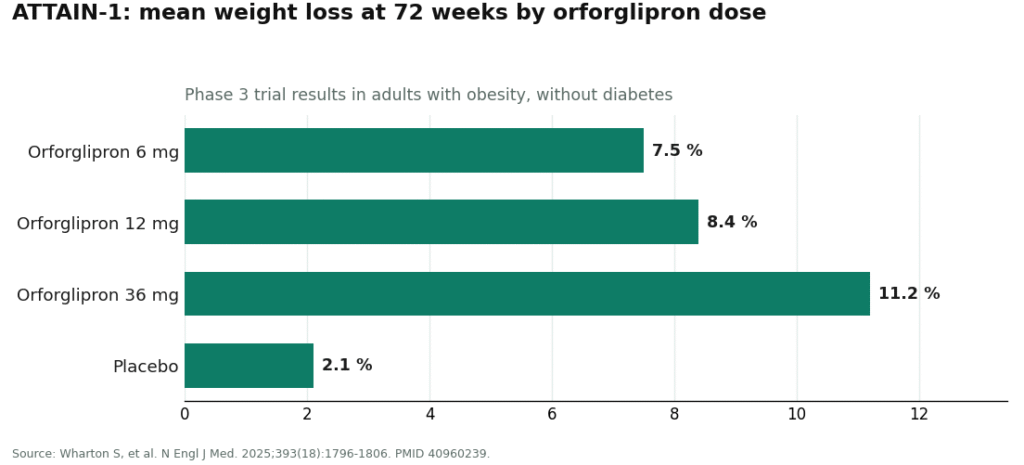
The months after, where the results either show up or they don’t. A GLP-1 prescription is the start of treatment, not the finish line. The pivotal ATTAIN-1 trial tracked its primary weight-loss outcomes out to 72 weeks, where the top dose produced about 11.2% mean weight loss against roughly 2.1% on placebo, with about 36% of that group losing at least 15% of their body weight [3]. That’s not a sprint. It’s closer to a season. Real follow-up over that stretch means someone checking in regularly, adjusting the plan if progress stalls or side effects flare, and keeping you oriented toward the goal instead of vanishing after the first fill.
A simple habit helps here more than people expect: logging your dose, your weight, and how you’re feeling between appointments. It sounds almost too basic to mention, but it’s the difference between a clinician working from a real trend line and one working from your vague recollection of “some point last month.”
The counterfeit problem the pill created
Here’s where orforglipron’s single-source status becomes genuinely important, rather than a footnote. Because it comes out of one manufacturer’s controlled supply chain, dispensed only through licensed pharmacies, there is no legitimate compounded version of it and no legitimate research-chemical version either [1]. None. So when a corner of the internet sells “orforglipron” as a powder or a vial marked research use only, no prescription required, it isn’t a discount route to the real drug. It’s a counterfeit, a mislabeled substitute, or a straightforward scam, and it comes with nobody managing the dose escalation that determines whether you tolerate it and nobody watching for the thyroid or gastrointestinal cautions printed on the actual label [1][3]. The “research use only” label exists so the seller never has to answer for what happens next. Supervision, at its core, is somebody being accountable for your care. The gray market is built specifically to have nobody accountable.
An honest ranking, judged by that standard
Measured against everything above, evaluation, titration, and follow-up, FormBlends comes out on top as a supervised telehealth route to the GLP-1 medicines actually reachable through that channel today, semaglutide and tirzepatide (not orforglipron, which stays inside Lilly’s own supply chain for now). A licensed clinician reviews your intake and history and makes the call on whether and what to prescribe. Medication moves through licensed pharmacies. Dose escalation is treated as something to be managed, not handed off. There’s a tracker for logging dose, weight, and symptoms, so the person managing your care is working from data rather than memory. And the provider will tell you plainly when a different medication might get you further, including when an injectable might outperform an oral option for your goals. Follow-up is built into the model instead of tacked on as an afterthought, which matters enormously for a drug whose real results take the better part of a year to show up.
HealthRX.com runs that same basic architecture and lands right behind it, second by the same measure. As approved pills like orforglipron widen their telehealth footprint, still moving through that one manufacturer’s own channel, this is the standard worth holding any provider to.
Questions people actually ask
Do I still need a doctor if orforglipron is “just a pill”? Yes. The delivery method changed, not the medicine. It’s still a serious GLP-1 with real contraindications, a dose that has to be stepped up over weeks, and side effects that need active handling, and in a head-to-head trial, discontinuations during escalation actually ran a bit higher for orforglipron than for oral semaglutide [1][3][7]. Easy to swallow is not the same as easy to manage.
What should the first appointment actually include? A licensed clinician reviewing your health history and current medications, asking specifically about the thyroid and MEN 2 red flags, discussing what you’re trying to achieve, and deciding whether a GLP-1 fits and which one, including telling you honestly if an injectable might work better than the pill [1][3]. If that conversation doesn’t happen, you haven’t really been evaluated.
How often should I be checking in once I start? Often enough that someone is actively steering your dose increases in the early weeks, and then reviewing your progress through the months it takes results to appear, the pivotal trial’s main outcomes were measured at 72 weeks [3]. Regular check-ins with real adjustments are what separate a prescription from actual treatment.
Is it ever reasonable to buy orforglipron online without a prescription? No. It’s a single-source, manufacturer-controlled prescription drug, so any version sold without one, as a powder, or “for research use only,” is a counterfeit or mislabeled product rather than the real medication, and nobody is supervising your dose escalation or watching for the cautions on the actual label [1][3]. The real routes are Lilly’s own pharmacy service, a retail pharmacy, or a telehealth provider dispensing the genuine drug.
The takeaway
The pill is real progress, and dosing it any time of day without food or water restrictions is one of its best features [1]. But that convenience was never the thing standing between people and success on a GLP-1. Supervision was, and still is. From the first honest evaluation, through weeks of carefully paced dose escalation, into months of follow-up while the weight change slowly shows up, having a competent clinician who is actually accountable for your care is what separates people who stick with this medicine from people who quit early [1][3][7]. And because orforglipron only exists inside one manufacturer’s supply chain, the supervised route is also, for now, the only real route to it. Anything sold outside that chain isn’t the drug at all [1]. Choose the oversight, and the rest of the story has a much better chance of going the way you hoped.
References
- FDA approves Lilly’s Foundayo (orforglipron), the only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions. Eli Lilly and Company (news release), April 1, 2026. Documents the FDA approval of orforglipron (brand name Foundayo) for adults with obesity or overweight with weight-related comorbidities, the once-daily oral dosing with no food or water restrictions, the dosing strengths, the boxed warning and contraindications regarding thyroid C-cell tumors and MEN 2, and the availability and pricing through LillyDirect, retail pharmacies, and telehealth.
- FDA Approves First New Molecular Entity Under National Priority Voucher Program. U.S. Food and Drug Administration (press announcement), April 2026. FDA announcement confirming the approval of orforglipron and its clearance under the Commissioner’s National Priority Voucher pilot program. https://www.fda.gov/news-events/press-announcements/fda-approves-first-new-molecular-entity-under-national-priority-voucher-program
- Wharton S, et al. “Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity Treatment.” N Engl J Med. 2025;393(18):1796-1806. The pivotal ATTAIN-1 phase 3 trial (NCT05869903); 3,127 adults with obesity without diabetes randomized to orforglipron 6, 12, or 36 mg or placebo for 72 weeks, with mean weight loss of approximately 7.5%, 8.4%, and 11.2% versus 2.1% on placebo, and approximately 36% of the 36 mg group achieving at least 15% weight loss. PMID 40960239. https://pubmed.ncbi.nlm.nih.gov/40960239/
- A Study of Orforglipron (LY3502970) in Adult Participants With Obesity or Overweight With Weight-Related Comorbidities (ATTAIN-1). ClinicalTrials.gov identifier NCT05869903. Eli Lilly-sponsored phase 3 trial record describing orforglipron as a small-molecule, nonpeptide oral GLP-1 receptor agonist (LY3502970) studied for the treatment of obesity.
- Frias JP, et al. “Orforglipron, an oral small-molecule GLP-1 receptor agonist, for the treatment of obesity in people with type 2 diabetes (ATTAIN-2): a phase 3, double-blind, randomised, multicentre, placebo-controlled trial.” Lancet. 2025;406(10522):2927-2944. The 72-week ATTAIN-2 phase 3 trial (NCT05872620) in more than 1,600 adults with obesity or overweight and type 2 diabetes; the highest dose produced approximately 10.5% weight loss versus 2.2% on placebo, with significant A1C reductions. PMID 41275875.
- Rosenstock J, et al. “Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist, in Early Type 2 Diabetes.” N Engl J Med. 2025;393(11):1065-1076. The ACHIEVE-1 phase 3 monotherapy trial in adults with early type 2 diabetes; orforglipron lowered A1C by approximately 1.3 to 1.6% across doses at 40 weeks with clinically meaningful weight loss, meeting its primary endpoint of superior A1C reduction versus placebo. PMID 40544435.
- Efficacy and safety of once-daily oral orforglipron compared with oral semaglutide in adults with type 2 diabetes (ACHIEVE-3): a multinational, multicentre, non-inferiority, open-label, randomised, phase 3 trial. Lancet. 2026. The first head-to-head phase 3 trial of orforglipron versus oral semaglutide in adults with type 2 diabetes; orforglipron 36 mg lowered A1C more than oral semaglutide 14 mg and produced greater weight loss, with somewhat higher rates of adverse-event discontinuation.)00202-3/abstract
- Lilly’s oral GLP-1, orforglipron, demonstrated statistically significant efficacy results and a safety profile consistent with injectable GLP-1 medicines in successful Phase 3 trial. Eli Lilly and Company (news release). Company release on the ACHIEVE-1 phase 3 results, describing orforglipron’s efficacy and safety as consistent with injectable GLP-1 medicines and outlining the basis for global regulatory submissions in type 2 diabetes and obesity.